Which ACL Graft Type is Best?
- The three main ACL graft types – BTB, hamstring, and quadriceps tendon – each have distinct trade-offs in pain, strength, and failure risk.
- Hamstring grafts have higher re-tear rates in young pivoting athletes, especially when graft size is under 8 mm.
- Adding a Lateral Extra-Articular Procedure (LEAP) significantly reduces re-tear risk and is unanimously recommended for active patients 25 and under receiving a hamstring graft.
- Graft choice should be individualized based on age, sport, and surgeon experience.
This is an age old question in surgery and rehabilitation. As a physical therapist and athletic trainer, I don’t make the surgical graft choice, but I do get to see the rehabilitation process, outcomes, and retear rates (including what is reported in the research). For almost all of my 30 years as a rehabilitation provider, I have been a staunch supporter of the original gold standard bone patellar tendon bone graft. That was until I talked with world-renowned surgeon Dr. Matt Daggett on the Rehab & Performance Lab Podcast ACL Graft Choice: Is There a New Gold Standard?
So that we are all on the same page, let’s take a look at the common graft choices and summarize their pros and cons according to Dr. Daggett.
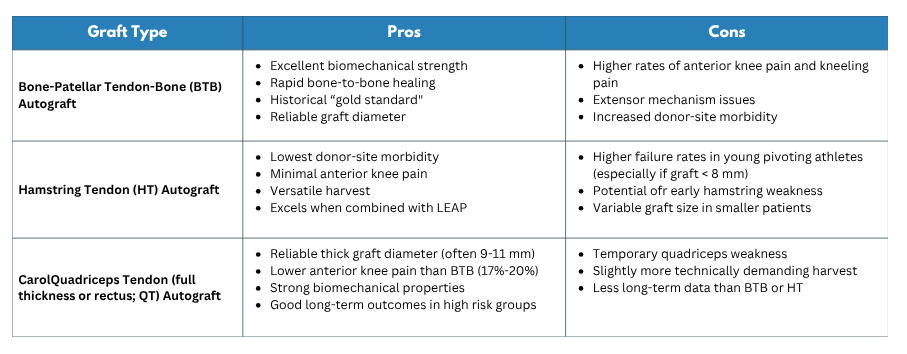
Common Graft Choices
Bone-Patellar Tendon-Bone Autograft - The Historical Gold Standard
This graft has excellent biomechanical strength with high bone-to-bone healing rates. Its consistent graft diameter makes it a reliable choice. The downside is not because of the graft itself, it is what happens where the graft is taken. There are much higher rates of anterior knee pain and extensor mechanism issues. These graft site issues can make regaining quad strength more challenging.
Hamstring Tendon Autograft - The Less Painful Alternative Graft
This graft is typically a quadrupled semitendinosus/gracilis muscle tendon. Where this graft excels is having much less harvest site pain and no anterior knee pain. This reduces the arthogenic muscle inhibition so that quad strength is returned much faster and more fully (which is important for sport and long term function) The downside of the hamstring graft is higher failure rates in young pivoting athletes (especially if the graft is less than 8 mm), potential for early hamstring weakness or stability motor control changes. Spoiler alert: The retear rate of this graft is substantially reduced if it is combined with a Lateral Extra-Articular Procedure.
Quadriceps Tendon - The Newer Kid on the Block
This graft can either be a full thickness quad tendon or just the rectus femoris. This graft produces a reliable thick graft diameter (9–11 mm) and has lower anterior knee pain than BTB but not as low as hamstring (Dr. Daggett is finding that rectus femoris graft has even less anterior knee pain). The quad graft also has strong biomechanical properties and good long-term outcomes in high-risk groups. The downside of this graft is quadriceps weakness and it is a slightly technically more demanding procedure, and there is less long-term data than BTB or HT. Personal side note, in the episode we talk about a theory of why I would prefer using the rectus femoris versus the full thickness quad tendon (hint: it involves using a stabilizing muscle versus a prime mover).
Which ACL graft should you choose? ACL Graft Choice Comparison
Graft choice should be made based on the patient presentation (age, body size), what sports/activities they are going back to, and the surgeon's technical abilities/preference for performing the surgery with a certain graft type. Listen to the episode for the full details on this.
Here is my biggest take away from Dr. Daggett in this episode – in order to reduce the re-tear rates, a lateral extra articular procedure should be performed in most cases. These are procedures that improve rotational stabilization and are performed along with the ACL reconstruction.
There are generally two primary types of LEAP : Anterolateral Ligament Reconstruction (ALLR) and Lateral Extra-Articular Tenodesis (LET). Here is how they compare structurally and clinically:
LET vs. ALLR: What’s the Difference?
Lateral Extra-Articular Tenodesis (LET): This is a non-anatomic procedure (often using the modified Lemaire technique). The surgeon takes a local strip of the iliotibial band (ITB) or gracilis tendon, passes it under the lateral collateral ligament, and fixes it to the tibia to create a protective sling. It is simpler, faster, and highly cost-effective. The trade-off? Minor lateral knee pain is slightly more common after surgery, though it is usually short term.
Anterolateral Ligament Reconstruction (ALLR): This is a true anatomic reconstruction. It uses a separate or combined graft (usually the gracilis) to recreate the native anterolateral ligament. While it is a bit more technically demanding for the surgeon and carries a slightly higher procedural cost, lateral pain post-op is less common.
The bottom line between the two? Their failure rates are about the same at around 3%, and their overall clinical outcomes are equivalent. They both get the job done.
What the Science Says: The 2025 LEAP International Consensus
This isn't just expert opinion or clinical intuition. The 2025 LEAP International Consensus (Part 2 can be found here), recently published in Arthroscopy, represents the highest level of global agreement on when to use these lateral procedures.
Here is the panel recommendation:
- 100% Unanimous Agreement: You must add a LEAP for active patients aged 25 or younger who are receiving a hamstring autograft ACL reconstruction. In this population, it is absolutely essential.
- Strong Consensus (90%–99%): You should add a LEAP if the patient presents with a high-grade (Grade 3) pivot shift, baseline knee hyperextension greater than 10° (remember, context matters – fear the asymmetry!), skeletal immaturity, a revision ACL reconstruction, or if they are returning to high-level pivoting and contact sports with multiple risk factors on board.
If you want more information on the clinical nuances of how we manage these athletes from initial graft selection all the way to return-to-sport testing, listen to the full discussion on the Rehab & Performance Lab Podcast. If you'd like CEUs, make sure to use the MedBridge link.












